Implementing health reform in the states is a governmental responsibility. But Kaiser Health News reported this week that states are turning to foundations to help them with the costs of implementing these reforms.
 This important work involves investing resources in promising initiatives that aren’t yet “government ready.” Foundations are uniquely equipped to provide seed funding to experimental and innovative programs before they are ready for governmental action.
This important work involves investing resources in promising initiatives that aren’t yet “government ready.” Foundations are uniquely equipped to provide seed funding to experimental and innovative programs before they are ready for governmental action.
Financing governmental duties has not traditionally been the role of a foundation. Governmental programs should be implemented efficiently, but asking foundations to pay for this implementation is drawing dollars away from the most important work of foundations.
 This important work involves investing resources in promising initiatives that aren’t yet “government ready.” Foundations are uniquely equipped to provide seed funding to experimental and innovative programs before they are ready for governmental action.
This important work involves investing resources in promising initiatives that aren’t yet “government ready.” Foundations are uniquely equipped to provide seed funding to experimental and innovative programs before they are ready for governmental action.On the other hand, funding governmental obligations leads to two unintended consequences.
First, it relieves governments of their obligation to justify to the public the expenditures they need to make to implement their programs. This always seems to lead to unrealistic public expectations about how much things costs, and problems down the road with funding them.Second, it takes limited foundation dollars away from innovation and experimentation. Not every foundation initiative will succeed, and that’s the point. While some fail quietly, many have changed the way we understand and address health problems in America. Some of the best fundamentally change American society for the better.
To name just three recent examples that illustrate this point, consider our 30 year history with HIV/AIDS, our emerging approaches to addressing the mental health epidemic, and our understanding of health disparities across populations and regions. The Robert Wood Johnson Foundation created the AIDS Health Services Program in 1986, five years after AIDS was first reported in the United States. It was also the same year that President Reagan first mentioned AIDS publically. While government responded slowly to the crisis, the RWJF initiative flourished and was responsible for enabling the Ryan White CARE Act, which wasn’t passed by Congress for four more years.
Foundations are also leading the way in breaking down the barriers between health care and mental health care. Primary and behavioral health “integration” emerged as a treatment strategy in the early 1990s, nurtured along by foundation investments. It took the federal government fifteen more years before it began to make a serious commitment to integration through passage of the Mental Health Parity Act in 2008, the Medicare Mental Health parity law in 2008, and the Affordable Care Act in 2010.Health disparities are underreported and poorly understood. This is because they often offer no “local angle” to a story, but can only be understood in the context of comparing one group or region to another. Such comparisons are easily dismissed as “apples to oranges” by local policymakers.
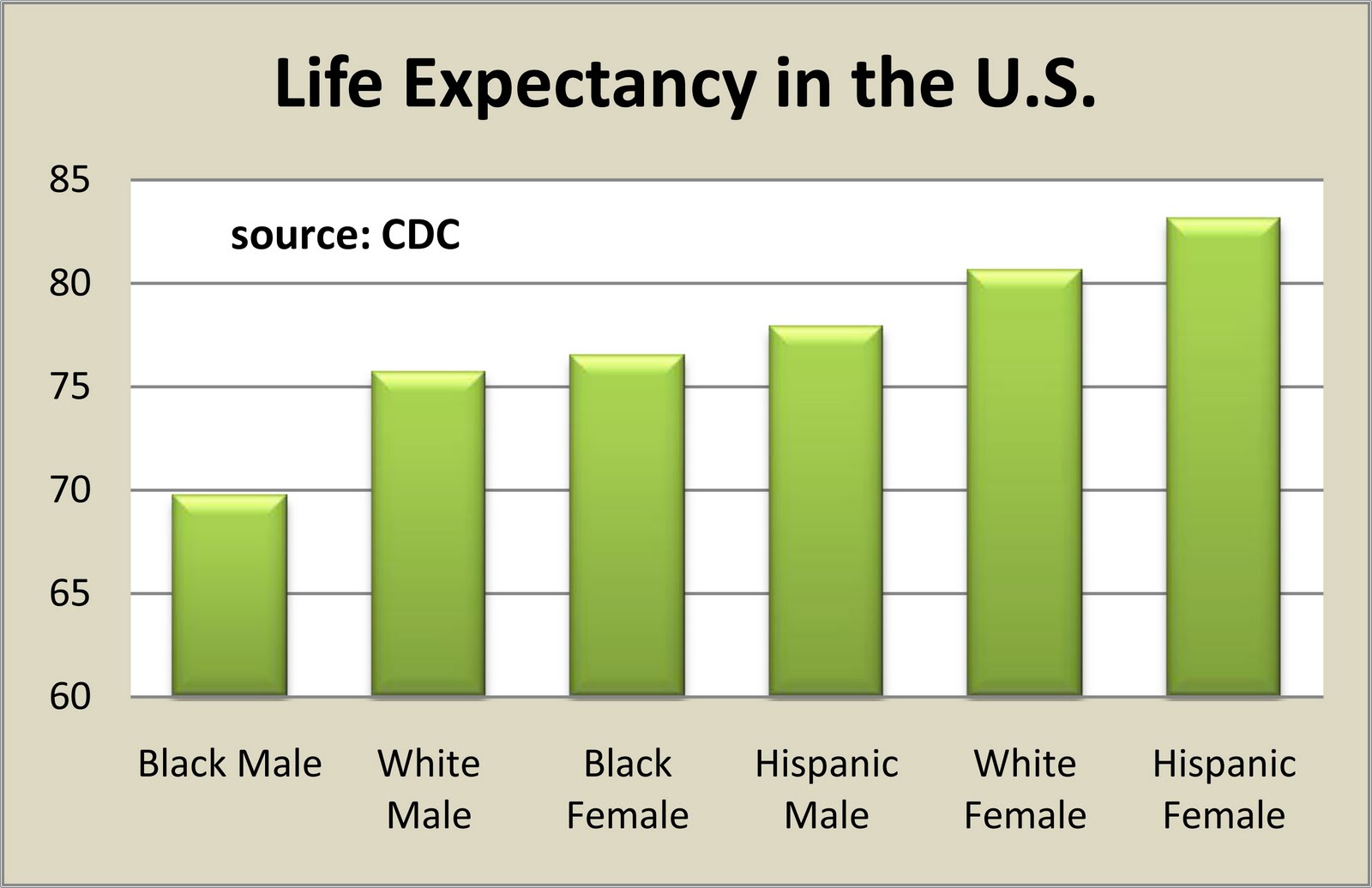
However, a government-supported university-based study shows vast and stunning differences in the life expectancies of various racial and geographic groups in the United States that can’t be so easily dismissed. The complete article, authored by Christopher Murray and others, is rich in comparative data, and its conclusions are more than troubling. Asian Americans in well-integrated counties have a life expectancy that is 15 years longer than African Americans living in urban settings sometimes just a few miles away. Rural white Americans in the Midwest have a 7 year life expectancy advantage over rural African Americans in the south.
Native American and African American men have life expectancies of between 60 and 70 years, but Asian American and white women living in rural areas have life expectancies well into their 80s. These numbers are underscored by readily-available CDC data tables. Nevertheless, the federal government did not make a major commitment to funding specific programs aimed at tackling disparities until more than four years after this study was published. Just recently, HHS announced its Promotores de Salud community health workers initiative, a strategy specifically designed to address health disparities in minority populations.
However, as Grantmakers in Health points out, both local and national foundations have been focused on this problem for years, leading the way by funding important initiatives looking at both populations and place as determinants of health status for many years. At their finest, foundations lead governments to action by experimenting with differing approaches to solving emerging policy problems, and finding and promoting those that work best.
It’s government’s job to bring them to scale. Then it can solve the underlying problems – like AIDS treatment and prevention, mental health and primary health care integration, and health disparities – it may have been too timid to address, either because it didn’t know what would work or because it didn’t know what the public would support.Asking foundations also to take on this job of government will reduce the dollars available for innovation and experimentation. The risk is that we miss out on finding an early solution to the next public health crisis.
To receive an email notifying you when new columns are published, please email gionfriddopaul@gmail.com. Want to find a source of data used in Our Health Policy Matters? Most data sources and past column charts can be accessed using the "data source" and "charts" tabs at the top of this page.
Comments
Post a Comment